
An evidence-based framework linking gait mechanics to actionable interventions.
1 Clinical Purpose
This protocol establishes a repeatable, field-ready methodology for assessing running gait using markerless motion capture. By utilizing the AiKYNETIX engine, practitioners can synthesize complex biomechanical data into clinical insights, facilitating targeted interventions and objective "Return-to-Play" (RTP) validation.
2 Target Users
- Sports Medicine & Rehab: Physical Therapists, Athletic Trainers, and Orthopedic Specialists.
- Performance Staff: Sports Scientists, Strength & Conditioning (S&C) Coaches.
- Institutional Athletics: High-performance centers, academies, and clinical gait labs.
3 The Diagnostic Hierarchy
AiKYNETIX deconstructs a running bout into a three-tiered analytical framework, moving from macro-level rhythm to micro-level joint kinematics.
- Tier 1: Spatiotemporal Parameters Foundational metrics including cadence, stride length, and Ground Contact Time (GCT). Used for rapid screening and establishing mechanical rhythm.
- Tier 2: Kinematic Profiles Detailed joint-angle time series across the gait cycle. Used for pattern recognition and identifying compensatory strategies.
- Tier 3: Advanced Biomechanical Insights Physics-derived loading proxies and movement quality indices. Used for deep-dive decision support and longitudinal trend tracking.
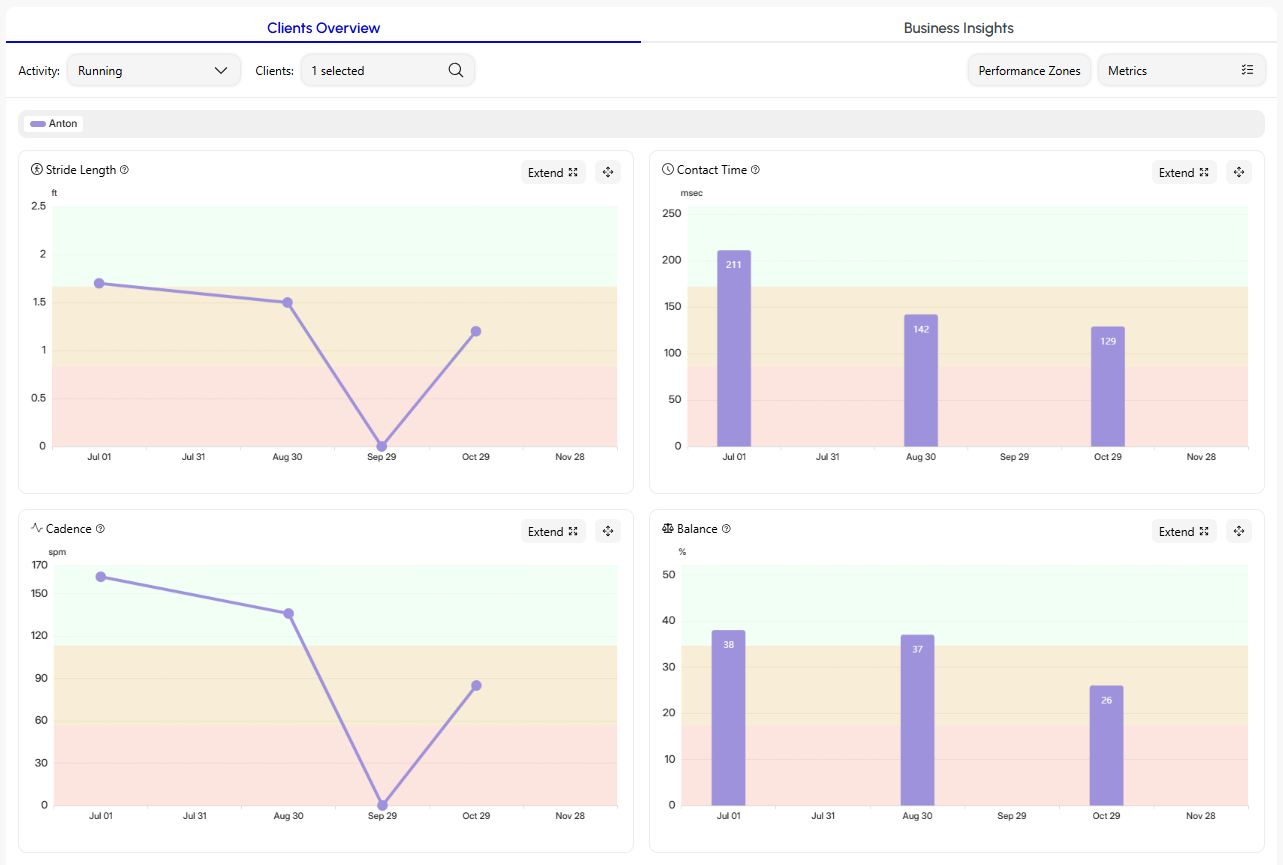
Fig 1. Interactive AiKYNETIX Web Dashboard: Spatiotemporal & Kinetic Overview.
4 Standard Operating Procedure (SOP)
To ensure data integrity and clinical reliability, follow this repeatable diagnostic loop:
- Data Acquisition: Record 20–60s of running (Sagittal view mandatory; Posterior view recommended for frontal plane analysis).
- Processing: Generate gait phase reports and joint-angle time series.
- Synthesis: Prioritize 3–5 key metrics against 1–2 specific kinematic patterns.
- Clinical Trial: Implement a specific intervention (e.g., verbal cueing, speed modulation, footwear change).
- Validation (Re-test): Standardize speed/setup and re-capture to quantify the mechanical delta.
- Longitudinal Tracking: Monitor weekly snapshots to identify trends in adaptation or fatigue.
5 Primary KPI Triage
Focus on these five sensitive metrics to drive clinical decision-making:
6 Clinical Pattern Recognition
Diagnosis should never rely on a single data point. Integrate metrics, time-series data, and the athlete’s subjective symptomology.
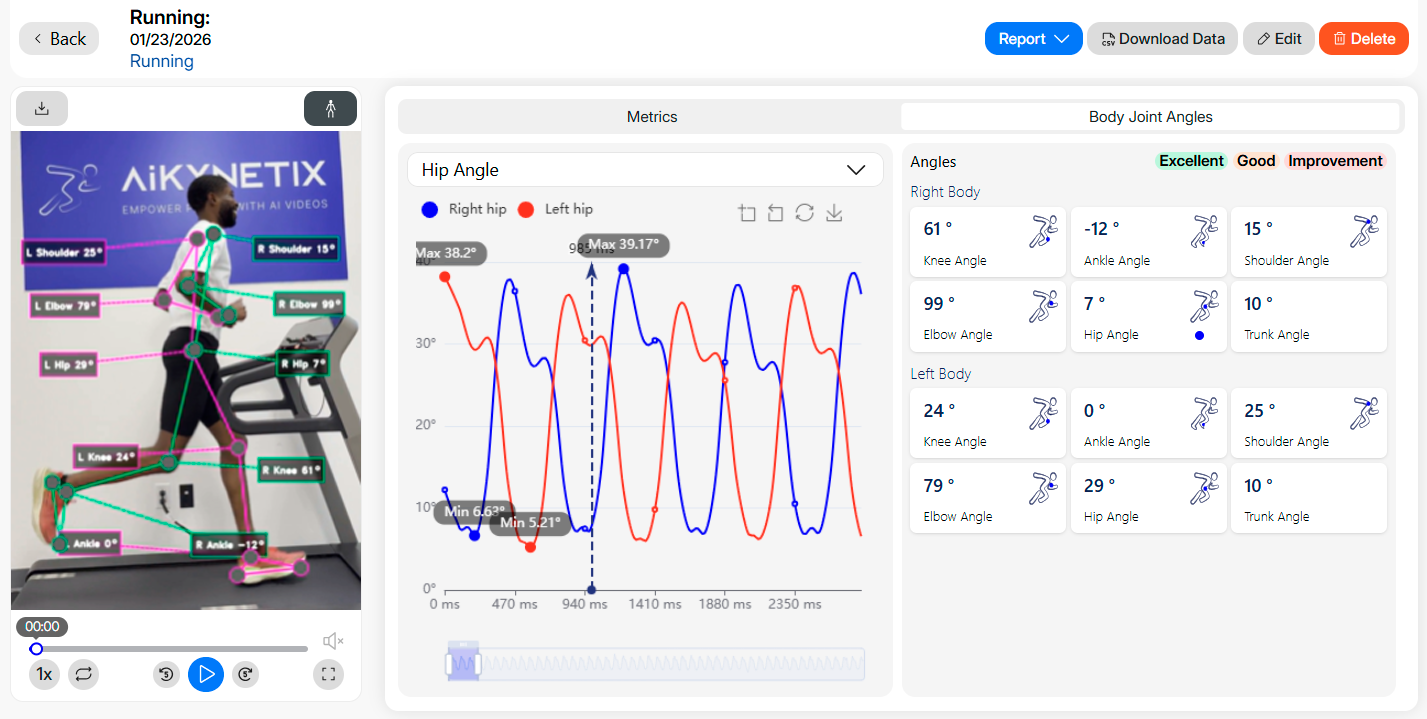
Fig 2. Multi-Joint Kinematic Tracking and Peak Angle Profiles in the AiKYNETIX Web Platform.
6.1 Mechanical Red Flags
- Persistent Asymmetry: Significant side-to-side variance suggests active guarding or incomplete rehab.
- Efficiency Decay: A simultaneous drop in cadence and rise in GCT at a constant speed indicates neuro-mechanical fatigue.
- Overstride Signature: Increased stride length with decreased cadence at a constant velocity.
6.2 Common Clinical Profiles
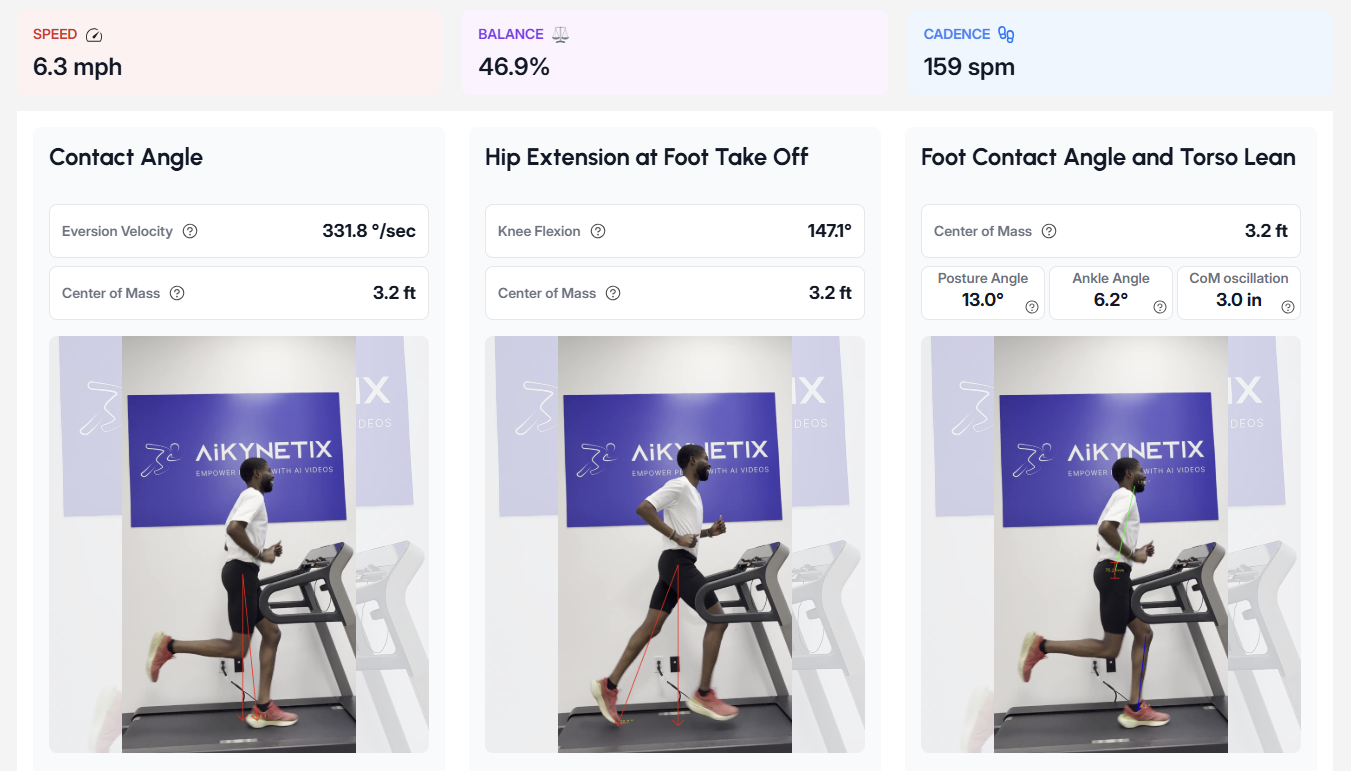
Fig 3. AiKYNETIX Advanced Biomechanical Insights: CoM Oscillation and Trunk ROM.
7 Intervention-to-Metric Mapping
Use this table to predict how specific "levers" will shift the athlete's mechanical profile.
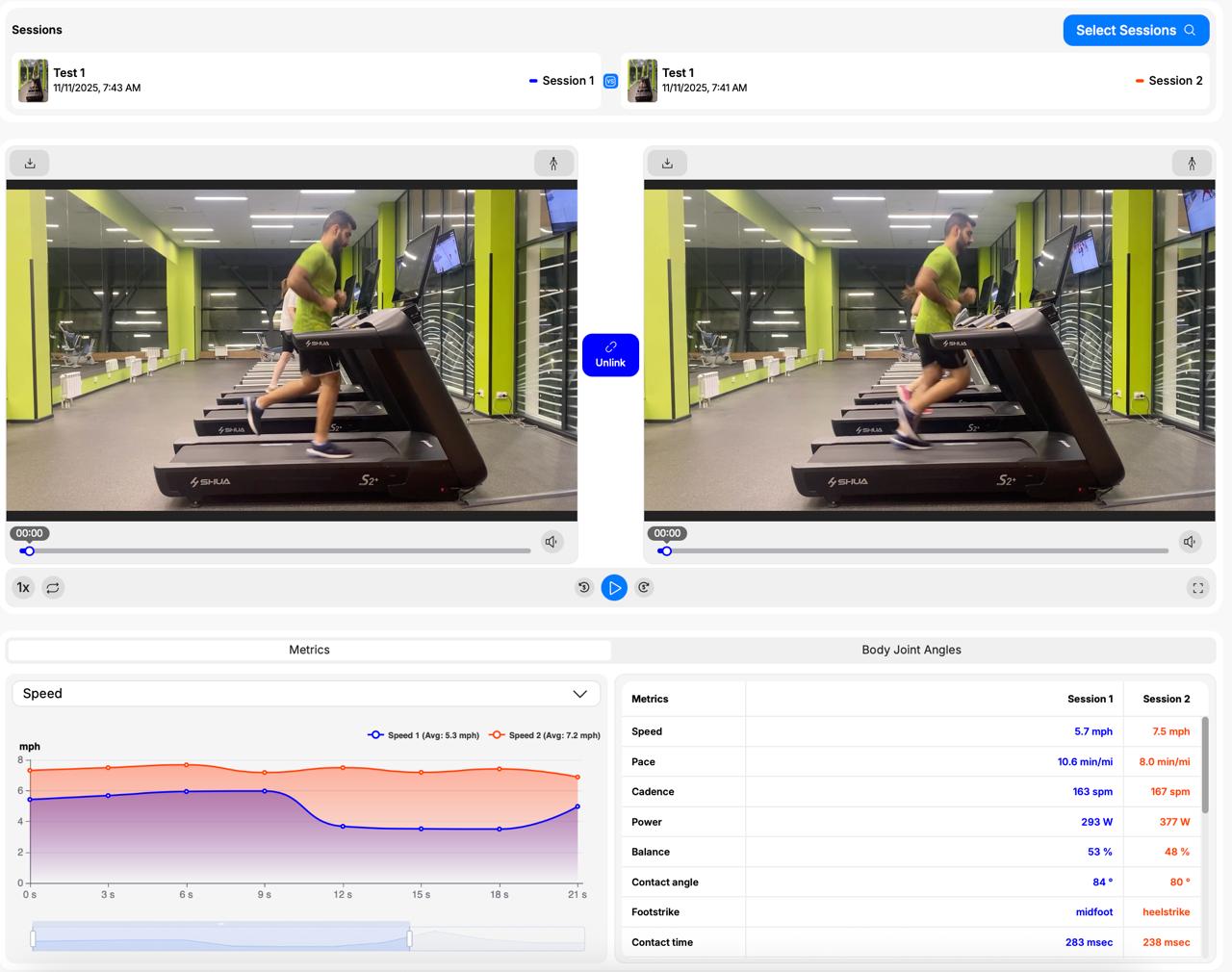
Fig 4. Longitudinal Analysis: Metric Delta Comparison Mode in the AiKYNETIX Web Platform.
8 Data Integrity & Filming Specs
To maintain "lab-grade" reliability in a field setting, adhere to the following specifications:
- Hardware: Tripod-mounted device, minimum 60 fps.
- Environment: Consistent, bright lighting; uncluttered background; no backlighting.
- Subject: Form-fitting athletic apparel to ensure clear visibility of joint centers.
- Framing: Full-body capture; do not truncate the distal extremities (feet/ankles).
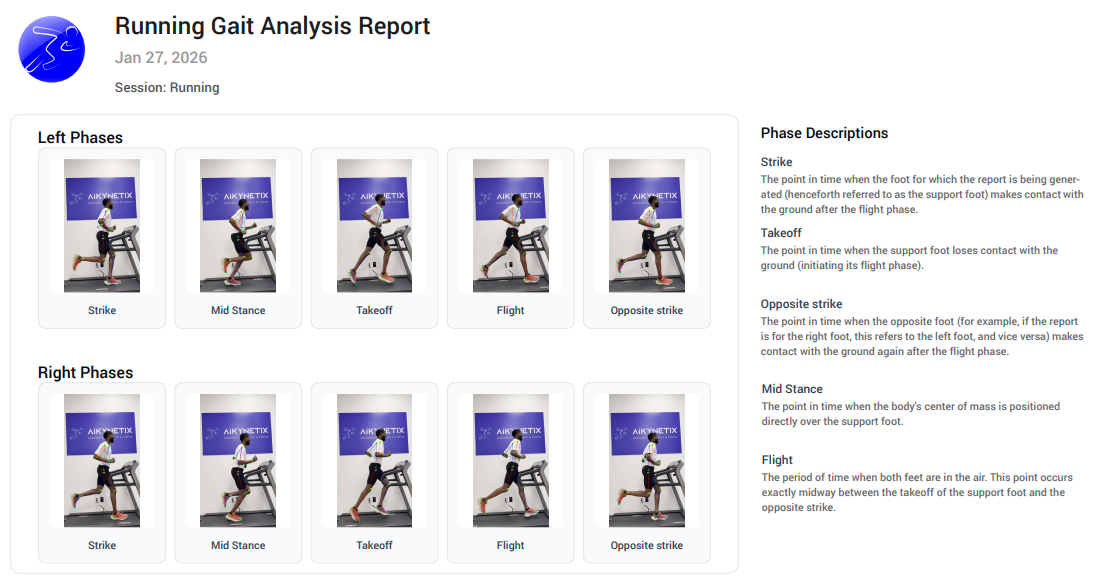
Fig 5. Automated PDF/HTML Clinical Diagnostic Report in the AiKYNETIX Web Platform.
Download your free PDF checklist to streamline your clinical workflow.
Want more tips like this?
📬 Subscribe to our newsletter for more practical guides!
📊 Start your free trial at aikynetix.app
📥 Got questions? Drop us a line: info@aikynetix.com
Find us in the socials:
Facebook | Instagram | X | Telegram | LinkedIn | Strava | YouTube
📬 Subscribe to our newsletter for more practical guides!
📊 Start your free trial at aikynetix.app
📥 Got questions? Drop us a line: info@aikynetix.com
Find us in the socials:
Facebook | Instagram | X | Telegram | LinkedIn | Strava | YouTube

